

Antimicrobial resistance poses a massive public health threat and is a priority for hospitals worldwide. Hospital teams must gather and analyze huge amounts of data on how doctors prescribe antibiotics and how patients respond. Singapore General Hospital is working with DXC Technology to use artificial intelligence (AI) to automate the process of auditing antibiotic usage to ensure optimal use and reduce hospital stays, mortality and readmission rates.
DXC and SGH co-created an AI model that gives antimicrobial stewardship program (ASP) teams faster, more accurate insights into antibiotic use. AI algorithms were built from patient data on the application of seven broad-spectrum intravenous antibiotics to treat pneumonia. Thousands of antibiotic prescriptions were subjected to a detailed clinical reasoning framework to quickly identify potential cases of misuse. The AI solution has been instrumental in helping ASP teams increase efficiency, which will enable SGH to realize its goal of having real-time information on each patient’s condition and recommending the most suitable type and method of treatment.
Antibiotic use
Overuse or misuse of antibiotics in hospital settings is a global problem, fuelling one of the most serious public health threats: antimicrobial resistance. An estimated 20 to 50 per cent of acute care hospitals worldwide aren’t prescribing antibiotics appropriately, and as a result, microorganisms become resistant to antimicrobials, including antibiotics, and can become superbugs that don’t respond to any drugs.
It is believed that up to 30 per cent of infections in hospitals in Singapore are resistant to third-generation cephalosporins, which are widely used broad-spectrum antibiotics. Reviews of Singapore hospitals have found that heavy use of broad-spectrum antibiotics has resulted in more resistance of Gram-negative bacteria. Further compounding the problem is a dwindling antibiotic pipeline, with limited therapeutics for the treatment of multi-drug resistant organisms (MDROs).
One key strategy to tackle the problem of antimicrobial resistance (AMR) is the use of antimicrobial stewardship programs (ASP). These initiatives seek to prevent the overuse of antimicrobial agents and ensure optimal selection of antibiotics, for example, where appropriate, making recommendations for the use of narrower-spectrum antibiotics and shorter durations of antibiotic use.
ASP teams have become well-established in Singapore’s public hospitals, and studies have shown they have been instrumental in improving antibiotic abuse. Crucially, their recommendations have led to shorter hospital stays, a reduction in mortality and readmission rates, and large cost savings for patients. High prescription rates of broad-spectrum antibiotics are understandable, since these are often seen as the easiest way to address infection. However, it’s important that good strategies are established to guide the use of antibiotics in a more precise and medically appropriate way.
Prescribing methodology
A key priority at acute care hospitals in Singapore, led by ASP teams and supported by precise, comprehensive data, is to establish a clear prescribing methodology.

The best approach for ensuring that this prescribing methodology will be put into practice is using automation and artificial intelligence (AI) to collate and analyse existing data. These technologies can significantly improve the ability of Singapore hospitals and the broader Singapore healthcare system to alleviate the overuse of antibiotics.
Antimicrobial efforts at Singapore General Hospital
One hospital that has a long-established ASP team is Singapore General Hospital (SGH), and studies have shown its recommended interventions have benefitted both patients and the hospital. Nevertheless, problems remain. In 2018 alone, approximately 12,000 audits performed for broad-spectrum antibiotic use at SGH showed that 20 to 30 per cent of these prescriptions were inappropriate. Yet this high volume of audits covered only seven intravenous antibiotics in the 2018 workflow, a small fraction of the range of antibiotics used in the acute hospital setting and in the wider community. To achieve comprehensive antibiotic stewardship, the ASP team would need to manually audit a wider range of antibiotics — both broad and narrow spectrum, delivered intravenously or through tablet form. This manual effort would exceed the manpower capacity of the ASP team.
Beyond simply auditing antibiotic use, the overarching goal is to shift the focus to an assessment of the clinical syndrome or type of infection, thereby adopting a more holistic and pre-emptive strategy to stewardship. This approach would typically include helping the prescribers systemically evaluate their patients’ presenting signs and symptoms as well as risk factors that affect antibiotic use. This would be a significant change from current practice (reactive strategy), where typically a patient will have been on an antibiotic for 3 days before the information needed to determine the right antibiotic for that patient has been collated.
A good starting point for a pre-emptive strategy is to focus on the most common type of infection treated at the hospital, pneumonia. According to SGH’s own studies, approximately 20 per cent of all infections treated in the hospital setting are due to pneumonia, and more antibiotic prescriptions are written for pneumonia than any other condition. However, not all pneumonias are due to bacterial infections. Some pneumonia types are due to viruses, for which antibiotics are not indicated. In addition, not all antibiotics need to be administered intravenously. In some cases, oral antibiotics are appropriate.
This underscores the need for a more patient-centered approach to be considered in stewardship efforts.
For example, the cost of treating pneumonia in a private hospital is more than $8,500 SGD and approximately $1,250 to $5,000 SGD in public hospitals for government-subsidized patients, with average lengths of stay of between 2 and 9 days. The potential for improved care and healthcare cost reduction is significant.
The ASP model: Pinpointing the right treatment
To tackle antimicrobial resistance and ensure that patients get the appropriate treatment, Singapore General Hospital’s ASP is developing a clinical reasoning framework for prescriptions based on five categories of questions, each with markers to assist with the diagnosis and selection of antibiotics:
- Is there an infection? This includes whether the patient has a fever; the patient’s haemodynamic status; findings from blood tests, such as white blood count, neutrophil count, monocyte count; sputum cultures; throat swab for respiratory viral panel; methicillin-resistant Staphylococcus aureus (MRSA) screening; etc. With pneumonia, for example, tests would determine whether the infection was viral versus bacterial.
- Where is the infection? What are the presenting complaints? What are the biomarkers from lab tests, X-rays, etc.?
- When did the infection occur? Did it occur less than 48 hours ago or more than 48 hours? This will help provide insight into whether it is a community-acquired infection or a hospital-acquired infection.
- Who is the host? What are the medical comorbidities of the patient (using the medical components within the Charlson Comorbidity Index)? Has the patient had a separate hospitalisation within 90 days? And does the patient have any allergies?
- What antibiotic should be selected? The previous four questions help to narrow down the selection of antibiotics. Further questions for the selection of treatment include: whether the patient has systemic inflammatory response syndrome (SIRS) or septic shock, has been in the intensive care unit (ICU), has taken antibiotics in the past 30 days, and has had any culture sensitivity reports concerning the bug and what it might be sensitive to.
This framework can help physicians achieve the objective of arriving at the right diagnosis. If the use of antibiotics is indicated, accurate data allows clinicians to select the narrowest spectrum antibiotic for the treatment of the infection for the right duration. The challenge for the ASP team has been to find a solution that enables them to access, leverage, analyse and act upon this vast amount of data.
To properly determine the type of infection and improve prescribing patterns, the ASP team will need to draw insights from multiple systems of record, first within the institution, then subsequently from national databases, if possible.
SGH Institution's propietary electronic medical records (EMR) system

In SGH, data will need to be drawn from institution’s proprietary electronic medical records system. Information from linked data repositories, such as radiology images, all laboratory results, histology reports and anaesthetic charts, is also required to support a syndromic approach for ASP.
High cost of antimicrobial review
This is a vast ecosystem to navigate and to prevent the inappropriate use of antibiotics, the ASP team as well as clinicians would need to have these insights in real time at the point of prescription.
By using AI to identify patient-cum-treatment profiles that require further review, the ASP team would be able to better prioritize complex cases, perform a more thorough analysis of each case prior to making recommendations on antibiotic choice and duration. Based on these recommendations, clinicians could then treat patients appropriately from the outset, and reduce the overprescribing of broad-spectrum antibiotics.
Automation would also enable the hospital to expand its audit coverage to a larger number of antibiotics prescribed in the hospital, thus increasing the service’s productivity, and also provide more thorough insight into the institution’s antibiotic consumption.
Managing a complex data model
Over the past four months, DXC and SGH have been co-creating an AI model that will enable faster, more accurate insights into antibiotic use and misuse, once certain data challenges are overcome.
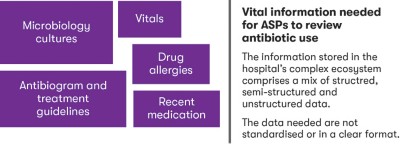
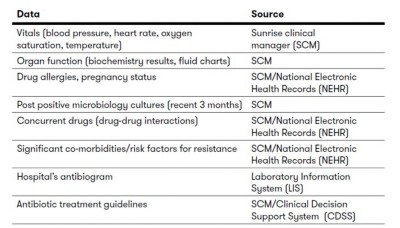
The teams developing the AI model must address problems of data quality, data engineering, data freshness and data completeness. The table below shows the disparate information within various systems.
Technical challenges
To tackle data quality issues, numerous data sets need to be categorized and processed. These challenges can be addressed through data engineering and data completeness strategies.
Data engineering transforms medical information collected at various points of the patient’s journey into useful components for analysis for the specific illness. For example, chronic illnesses are considered through the patient’s lifetime whether the diagnosis was made 1 month ago or 10 years ago. In contrast, lab test results for microbiology will only be considered valid if symptoms are presented within 3 months.
Data-completeness strategies address missing information, which is needed by the model. These could be due to the absence of an ordered test by the physician or lack of records. These strategies range from averaging out the missing information to computing a proxy based on other patient medical factors.
Addressing these technical challenges is integral to enabling AI models to be embedded within the hospital system. Once embedded and accessible to the ASP team and doctors, the potential to significantly improve antibiotic prescribing patterns can be realized.
Improving antibiotic stewardship unit oversight
Despite the challenges with data, DXC and SGH have made significant progress with the creation of an AI model for antibiotic analysis.
The first phase of the process was to build a model from ASP’s data set based on seven broad-spectrum intravenous antibiotics commonly used in the treatment of pneumonia.

Each antibiotic prescription was subjected to the clinical reasoning framework detailed above where the five categories of questions were used to determine the presence of an infection, understand the patient, and determine previous illnesses and treatments with antibiotics. The data was summarized based on the patient displaying any signs of symptoms within the relevant period. Additional information such as the number of days between patient admissions, administration of the pneumonia regimen was computed and included in the model.
Manual vs. AI
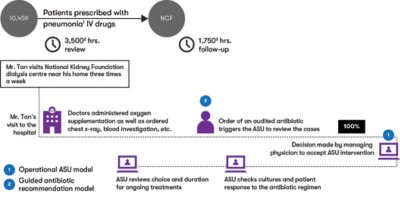
Through the use of AI algorithms, the teams have been able to achieve some important efficiencies, moving the hospital closer to the objective of real-time information on the patient’s condition and the most suitable type and method of treatment. Existing standard operational procedures of the ASP involve the manual review of all audited antibiotics for pneumonia, out of which 4 per cent required intervention from the ASP team in the form of alternative antibiotic treatments.
Within this process, there are two key decisions the ASP team needs to make.
The first is the review of the cases to decide whether the treatment is appropriate (operational AI model).
The second decision happens when a pneumonia treatment is deemed inappropriate, requiring intervention. The decision must be made to prescribe a suitable regimen of antibiotics (recommender AI model).
The operational AI model identities treatment profiles that require additional review and can narrow down the number of cases requiring immediate attention by the ASP team. In a test using 2,012 pneumonia treatments unseen by the model, 624 cases were flagged as requiring additional review. Seventy-two (87%) of all intervention cases were captured within the 624 cases flagged for review. Essentially, the model reduces the number of cases for review by a factor of three (624 out of 2,012) and increases the possibility of identifying cases requiring intervention within the prioritized cases three times — 11.5% — as compared to the full review process, which identifies 4% of all cases for intervention.
The recommender AI model suggests the appropriate antibiotics for each case and can be used to provide guidance to clinicians at the point of prescription. Due to the large number of possible antibiotic regimens, the recommender model was able to recommend the correct regimen only 50% of the time.
Speed of data analysis is also important to the success rate. While manual processes typically take 20 minutes to review each case, AI can assess the same data in less than a second, allowing the ASP teams to assess more data in real time for more antibiotics. This could mean reviewing more cases and expanding the ASP coverage to a larger set of antibiotics.
The next phase
The next goal is to gather more and deeper insights across all antibiotics to treat pneumonia and further enhance operational efficiency. By the third phase, the objective is to have those insights to help treat all infectious diseases with high levels of operational efficiency, providing a platform to support the overarching goal: right prescription, right dosage, right delivery at the right time for the right duration.
To move this objective forward and achieve a comprehensive and powerful AI tool to address antibiotic overuse and misuse, DXC and SGH will need to access a broader data set, including community data.
The ultimate goal is to have the automated system integrated with the hospitals’ current clinical systems, so prescribing decisions can be supported at the point of care. Consequently, the hospital will be able to prevent inappropriate use of antibiotics and develop more personalized treatment regimens that take into account each patient’s biomarkers, symptoms, comorbidities and medical history.
Proposed project plan
Value proposition — AI aid for antimicrobial prescription

Addressing a global health epidemic
The problem of antimicrobial resistance undoubtedly needs a global response. In Asia-Pacific and beyond, Singapore is recognized as a center of excellence. Leadership provided in Singapore to tackle the problem through progressive antimicrobial stewardship programs, supported by AI and automation, will pave the way for other markets to adopt similar strategies and improve global antimicrobial stewardship. Furthermore, holistic adoption of such an approach can greatly enhance situational awareness of prescription practices and use of antibiotics.
Learn more about DXC Analytics and Engineering.
Learn more about DXC in Healthcare.
About the authors
Andrea Kwa Lay Hoon, Assistant Director, Pharmacy (Research) and Pharmacy Clinician Scientist, Singapore General Hospital (SGH)
Jasmine Chung Shimin, Infectious Disease Physician, SingHealth Duke-NUS Transplant Centre
Winnie Lee, Pharmacy Specialist, SGH Pharmacy
Sarah Tang, Specialist Pharmacist, SGH Pharmacy
Lun Yi Tan, Executive, Clinical Quality & Performance, SGH Management
Yiling Chong, Senior Data Scientist
Akshay Saigal, Head of Innovation Labs, Asia, DXC Technology
Akmal Faiz Bin Omar, Data Scientist, DXC Technology